Advanced/metastatic breast cancer
What is advanced/metastatic breast cancer (a/mBC)?
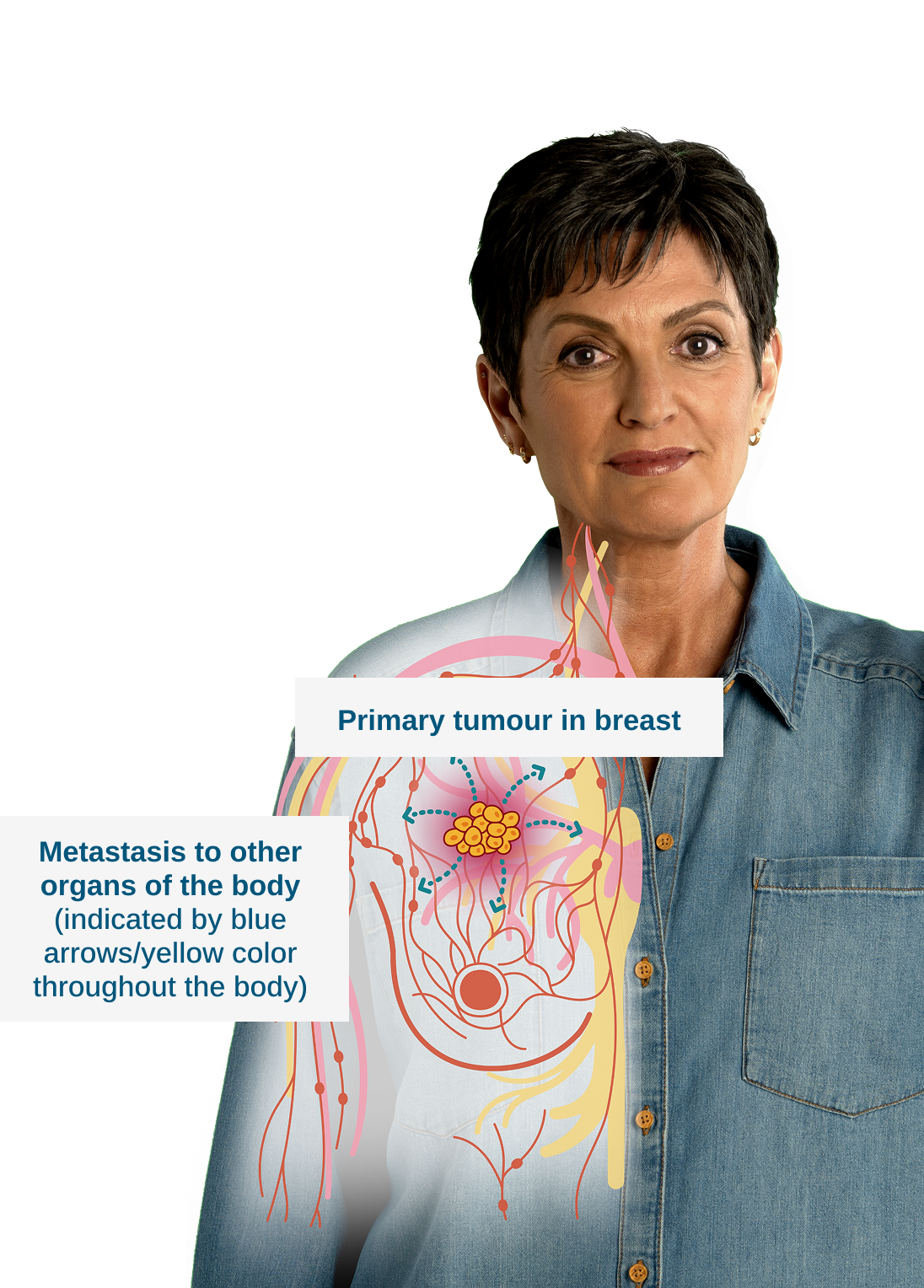
Also known as advanced, or Stage IV breast cancer,1,2 a/mBC is when the breast cancer has spread (metastasized) to other areas/organs of the body, such as the lungs, bones, liver and brain.1,2
What are
metastases?
Tumors at distant sites other than the original cancer site (e.g. breast) are called metastases.1




What are estrogen and progesterone?
Estrogen and progesterone are hormones related to female and male characteristics.1 Some tumors grow in response to these hormones by interacting with estrogen receptors (ERs) or progesterone receptors (PRs) in tumor cells.1
a/mBC treatment goals

Prolonging life1

Maximizing quality of life1
Hormone receptor-positive (HR+) tumors
Tumors with either or both hormone receptors, ER and PR, are known as hormone receptor-positive (HR+) tumors.1 ER+ tumors can be either ER+ or ER+ and PR+.1
Human epidermal growth factor receptor 2 (HER2) in a/mBC
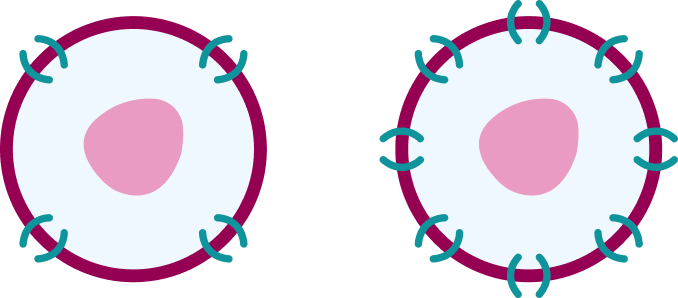
HER2 is another receptor present on all cells.1 It is involved in normal cell growth, multiplication, and repair.1 Around 20% tumors have high levels of HER2 and are known as HER2-positive (HER2+) tumors .1 Cancers with normal amounts of HER2 are known as HER2-negative (HER2-) tumors.1
Types of mBC
You might have heard about different types of a/mBC. These are classified according to the presence of HR and/or HER2 – each with outcome and treatment success predictive properties.1
Luminal A
(HR+/HER2-)1
Luminal B
(HR+/HER2- OR HR+/HER2+)1
HER2-enriched
(HR+/HER2+ OR HR-/HER2+)3
Triple-negative
(HR-/HER2-)1
Prevalence and outcomes
Most breast cancers (~75%) are ER-positive. Luminal A tumors are ER-positive and Luminal B tumors are mostly ER-positive.1,4 ER-positive tumors, relative to other breast cancer subtypes, are slow growing and tend to be less aggressive.3,5 In contrast, HER2+ tumors grow faster and are more likely to spread than HER2- tumors.1
Treatment of a/mBC

Key factors for treatment decisions
The presence of biomarkers including hormone receptors (HR) and/or HER2 in a tumor is a major factor in determining the most effective treatment.1
Systemic therapy
Systemic therapy is a treatment that enters the bloodstream and reaches the entire body.1 Sometimes, it is also combined with radiotherapy.1
Endocrine (hormonal/anti-hormonal) therapy for ER+/HER2- a/mBC
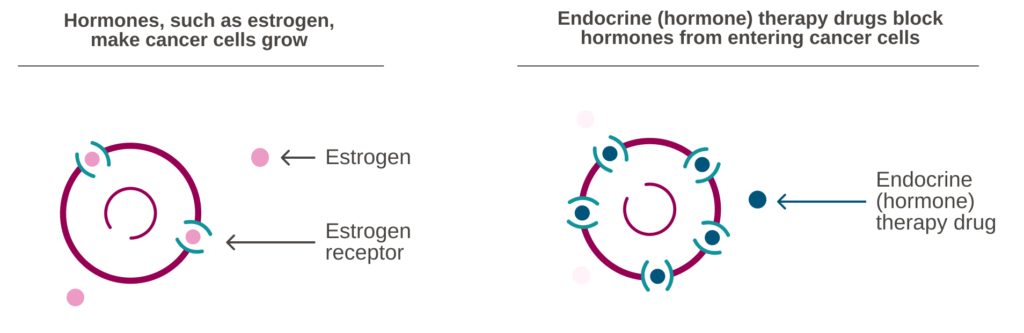
In ER+ breast cancer, estrogen causes over-stimulation of the pathways involved in the growth and multiplication of breast cancer cells (abnormal ER signaling).4
Inhibiting estrogen signaling may slow the growth of cancer cells.4
For most patients with ER+/HER2- a/mBC, the initial therapy is typically endocrine therapy, which aims to reduce the effects of estrogen by either blocking ERs on breast cells, reducing the number of ERs, or reducing the production of estrogen.1
It is taken alone or in combination with an additional treatment known as a CDK4/6 inhibitor.1

Endocrine therapy for ER+/HER2- a/mBC
Endocrine therapies
Endocrine (hormone) therapies aim to reduce the effects of estrogen by blocking the ER or limiting the levels of estrogen in the blood, e.g:1
- Selective Estrogen Receptor Modulators (SERMs) block ER signaling in the breast
- Selective Estrogen Receptor Degraders (SERDs), such as fulvestrant, block the ER and also reduce the number of ERs in the cell
- Selective Estrogen Receptor Degraders (SERDs) block the ER and also reduce the number of ERs in the cell
- Aromatase Inhibitors (Als), such as anastrozole, letrozole and exemestane, reduce the production of estrogen in tissues and organs beyond the ovaries
- Aromatase Inhibitors (Als) reduce the production of estrogen in tissues and organs beyond the ovaries

CDK4/6 inhibitors
Cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors are a type of targeted therapy.1
Targeted therapies block specific signaling pathways in cancer cells, in this case CDK 4 and 6 proteins, that help them grow.1

a/mBC: advanced/metastatic breast cancer; CDK4/6: cyclin D kinase 4 and 6; ER: estrogen receptor; HER2: human epidermal growth factor receptor 2; HR: hormone receptor; PR: progesterone receptor.
- ESMO. Breast Cancer: A guide for patients. Accessed October 2025. Available at: https://www.esmo.org/content/download/6593/114959/1/EN-Breast-Cancer-Guide-for-Patients.pdf.
- Johns Hopkins Medicine. Health: Conditions and diseases: metastatic breast cancer. Accessed October 2025. Available at: https://www.hopkinsmedicine.org/health/conditions-and-diseases/breast-cancer/metastatic-breast-cancer.
- BreastCancer.org. Molecular subtypes of breast cancer. Accessed October 2025. Available at: https://www.breastcancer.org/types/molecular-subtypes.
- Miziak P, et al. Cancers (Basel). 2023;15(19):4689.
- American Cancer Society. Breast cancer. Breast Cancer Hormone Receptor Status. Accessed October 2025. Available at: https://www.cancer.org/cancer/types/breast-cancer/understanding-a-breast-cancer-diagnosis/breast-cancer-hormone-receptor-status.html.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast Cancer Version 1.2026. ©National Comprehensive Cancer Network, Inc. 2025. All right reserved. Accessed February 2026. To view the most recent and complete version of the guideline, visit NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.