ESR1 mutations…
…are a majormain driver of endocrine resistance
ESR1 mutations acquired during ET may result in the development of endocrine resistance.ESR1 mutations can cause constitutive estrogen-dependent activation of the estrogen receptor.1-4

…are associated with poor outcomes
ESR1 mutations can produce a more aggressive disease that may adversely affect outcomes.ESR1 mutations lead to shorter survival in comparison with patients with wild-type ESR1.5,6

…may help driveinform treatment decisions
The tumour biomarker profile may influence the choice of therapy in 2L+.5,7,8
…are a majormain driver of endocrine resistance
ESR1 mutations acquired during ET may result in the development of endocrine resistance.ESR1 mutations can cause constitutive estrogen-dependent activation of the estrogen receptor.1-4
…are associated with poor outcomes
ESR1 mutations can produce a more aggressive disease that may adversely affect outcomes.ESR1 mutations lead to shorter survival in comparison with patients with wild-type ESR1. 5,6
…may help driveinform treatment decisions
The tumor biomarker profile may influence the choice of therapy in 2L+.5,7,8
Endocrine resistance in ER+/HER2- a/mBC
In postmenopausal women and adult men with ER+/HER2- advanced/metastatic breast cancer (a/mBC), ET + a CDK4/6i is standard of care.7,9


Several studies show that patients may progress on this treatment due to the acquisition of resistance mutations (also called acquired mutations) in tumour cells.1-4
Types of endocrine resistance
Resistance to endocrine therapy (ET) in ER+/HER2− a/mBC can be classified by clinical and molecular variables.10-13
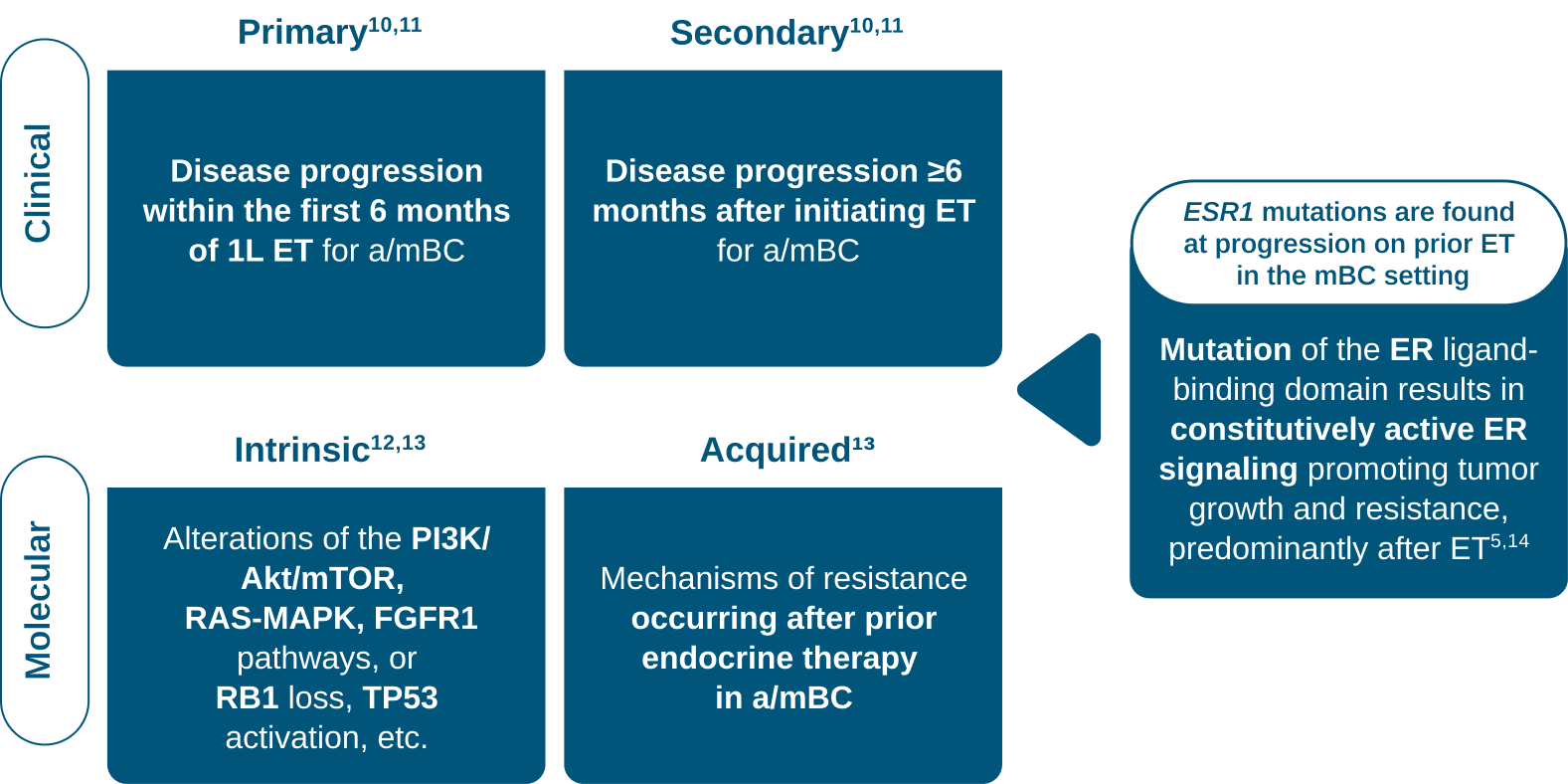
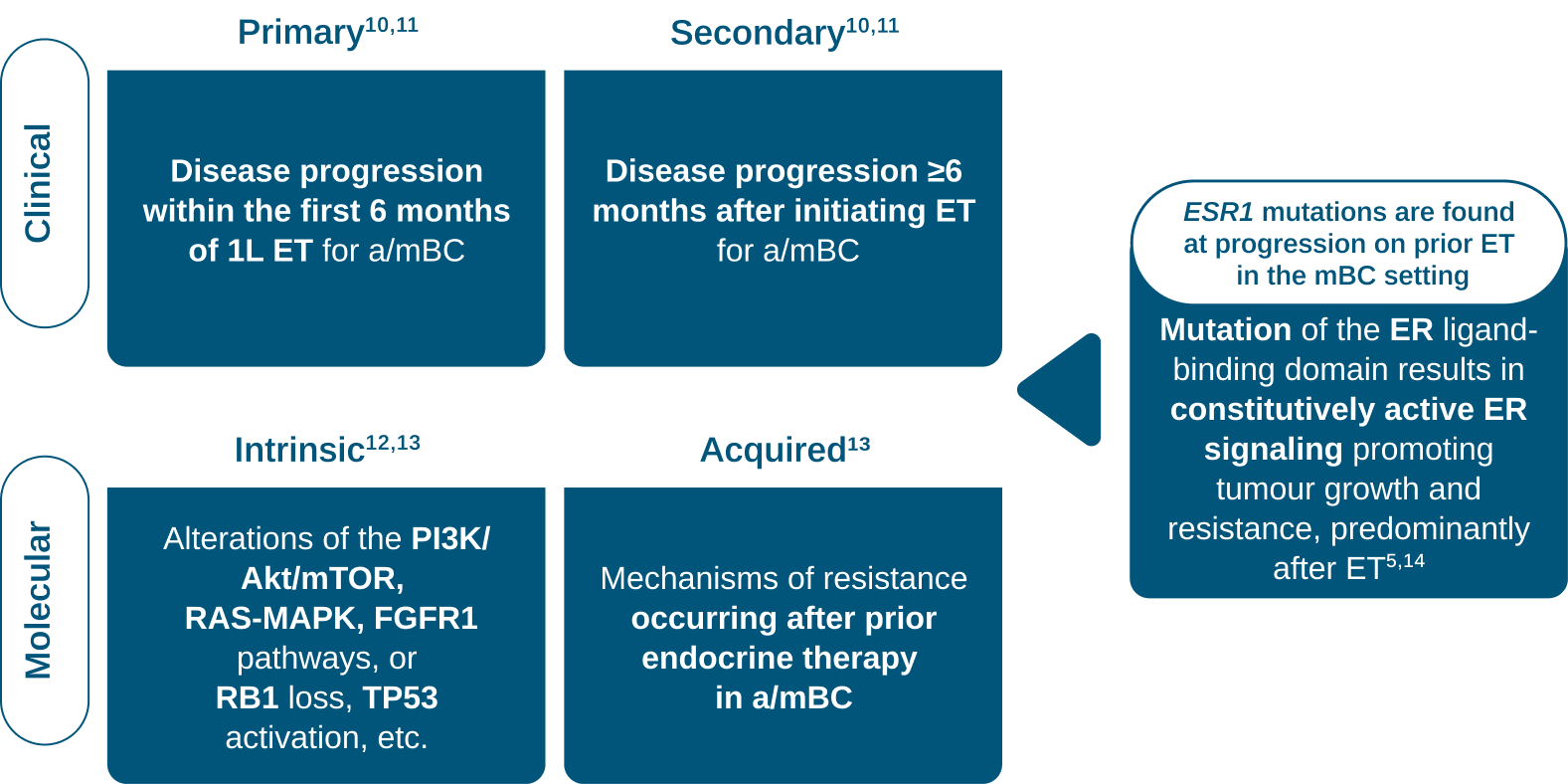
Resistance to conventional ET
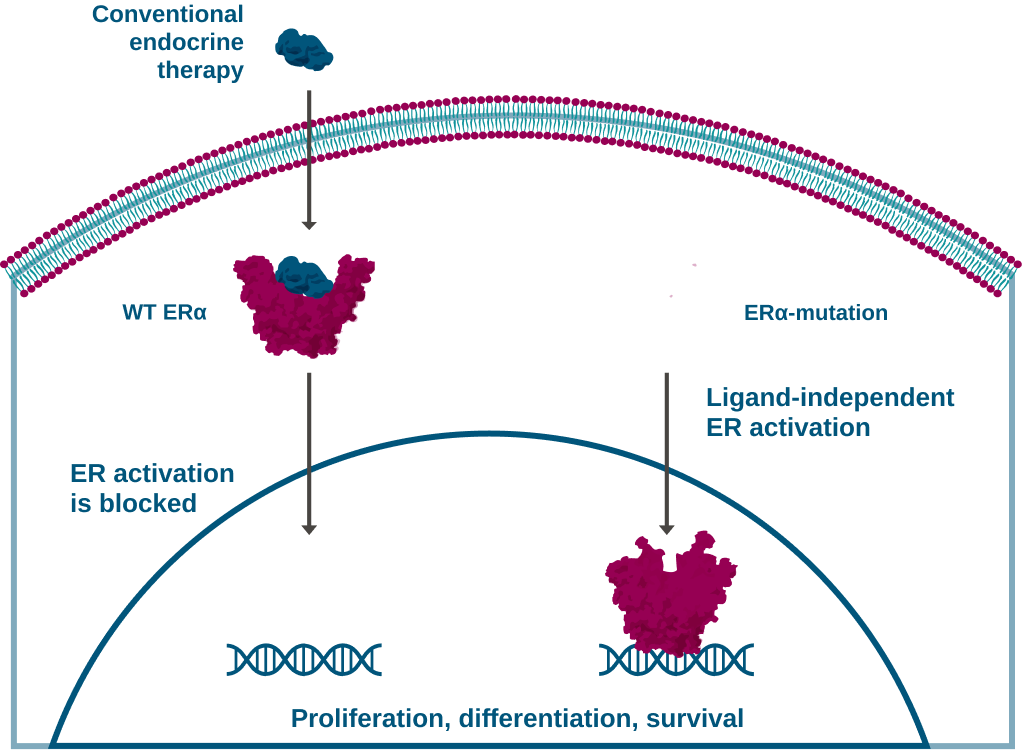
ET such as tamoxifen, aromatase inhibitors (AIs) and fulvestrant exert their antitumour activity by modulating the activation of the ER thus inhibiting the activation of downstream targets.5,15
By altering the ligand-binding domain, ESR1 mutations can also causemay cause endocrine resistance to conventional ET.5,15
Conventional endocrine therapies exert their antitumor activity by modulating the activation of the ER thus inhibiting the activation of downstream targets.5,15
By altering the ligand-binding domain, ESR1 mutations can also cause endocrine resistance to ET.5,15
Poor outcomes associated with ESR1 mutations

Patients with ESR1 mutations have significantly faster disease progression and worse survival outcomes (OS, PFS) as the accumulation of mutations can generate a more aggressive disease phenotype.1-6
The need to test for ESR1 mutations

Identification of patients with ESR1 mutations can help inform treatment decisions.5,7,8
Identification of breast cancer tumours with ESR1 mutations can help inform treatment decisions.5,7,8
For patients with a/mBC whose tumours harbour ESR1, PIK3CA, or AKT1 genetic alterations, existing and emerging targeted therapies are available.16-19
Routine ESR1 mutation testing at each disease progression is therefore important to inform appropriate treatment decisions.*,16
*Repeat ctDNA testing may be approriate following a further line of endocrine therapy and subsequent disease progression as long as the previous test was negative and the patient remains eligible as per NICE recommendation (TA1036).
1L: first-line; 2L: second-line; AI: aromatase inhibitor; AKT: protein kinase B; AKT1: AKT serine/threonine kinase 1; a/mBC: advanced/metastatic breast cancer; CDK4/6i: cyclin dependent kinase 4/6-inhibitor; ERα: oestrogen receptor alpha; ER+/HER2-: oestrogen receptor-positive/human epidermal growth factor receptor 2-negative; ESR1: oestrogen receptor 1; ET: endocrine therapy; FGFR1: fibroblast growth factor receptor 1; mTOR: mammalian target of rapamycin; mut: mutation/mutated; OS: overall survival; PFS: progression-free survival; PI3K: phosphoinositide 3-kinase; PIK3CA: phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; Ras-MAPK: mitogen-activated protein kinase; RB1: retinoblastoma tumour suppressor gene; TP53: tumour protein 53; WT: wild type.
- Clatot F, et al. Breast Cancer Res. 2020;22(1):56.
- Chandarlapaty S, et al. JAMA Oncol. 2016;2(10):1310.
- Turner NC, et al. Clinical Cancer Res. 2020;26(19):5172–7.
- Zundelevich A, et al. Breast Cancer Res. 2020;22(1):16.
- Brett JO, et al. Breast Cancer Res. 2021;23(1):85.
- Liao H, et al. Front Oncol. 2020;10:587671.
- Burstein HJ, et al. J Clin Oncol. 2023;41(18):3423–5.
- Hartkopf AD, et al. Breast Care (Basel). 2020;15(4):347–54.
- Gennari A, et al. Ann Oncol. 2021;32(12):1475–95.
- Rasha F, et al. Mol Cell Endocrinol. 2021;532:111322.
- Patel R, et al. NPJ Breast Cancer. 2023;9:20.
- Rani A, et al. Front Endocrinol (Lausanne). 2019;10:245.
- Xu P, et al. Acta Pharmacol Sin. 2021;42:171–8.
- Toy W, et al. Nat Genet. 2013;45(12):1439–45.
- Bardia A, et al. N Engl J Med. 2018;379(20):1946–53.
- Rugo HS, et al. Clin Adv Hematol Oncol. 2023;21(12):623−32.
- Clinicaltrials.gov. NCT04975308 (EMBER-3). Accessed May 2026. Available at: https://clinicaltrials.gov/study/NCT04975308.
- Goetz MP, et al. Ann Oncol. 2023:34(12)1141−51.
- Raheem F, et al. Int J Mol Sci. 2023:24(22):16198.