For ESR1 mutation testing…
…international guidelines recommend liquid biopsy as the preferred testing methodology
Blood circulating tumour DNA (ctDNA) testing has a high sensitivity for ESR1 mutations.1

…archival primary tumour tissue should not be used
ESR1 mutations acquired due to prior ET are rarely present in primary tumour tissue.2
…international guidelines recommend liquid biopsy as the preferred testing methodology
Blood circulating tumour DNA (ctDNA) testing has a high sensitivity for ESR1 mutations.1
…archival primary tumour tissue should not be used
ESR1 mutations acquired due to prior ET are rarely present in primary tumour tissue.2
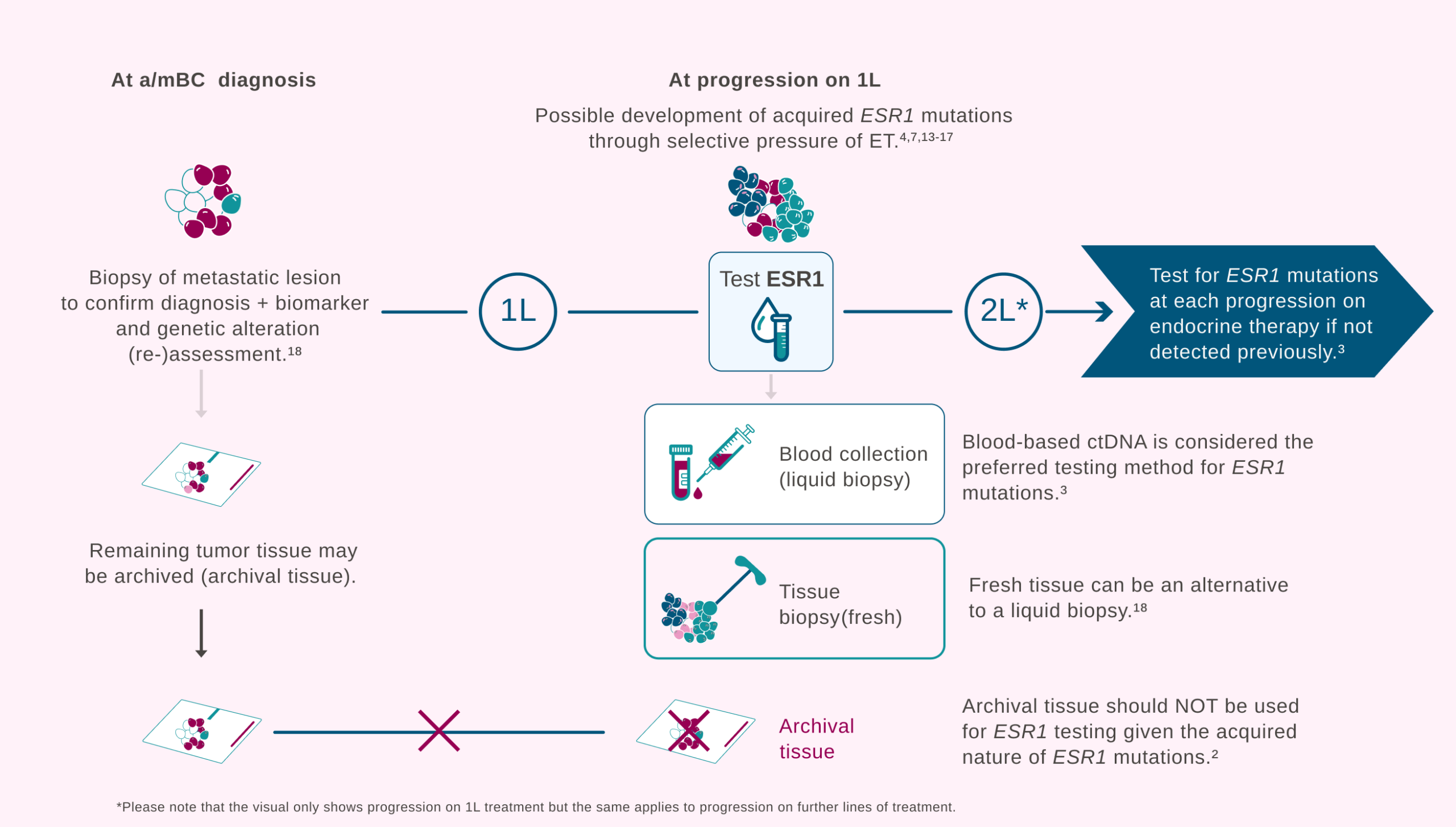
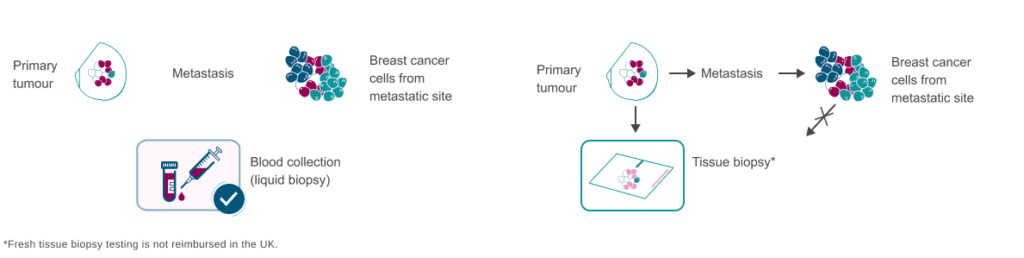
Liquid biopsy is the preferred testing methodology to detect ESR1 mutations
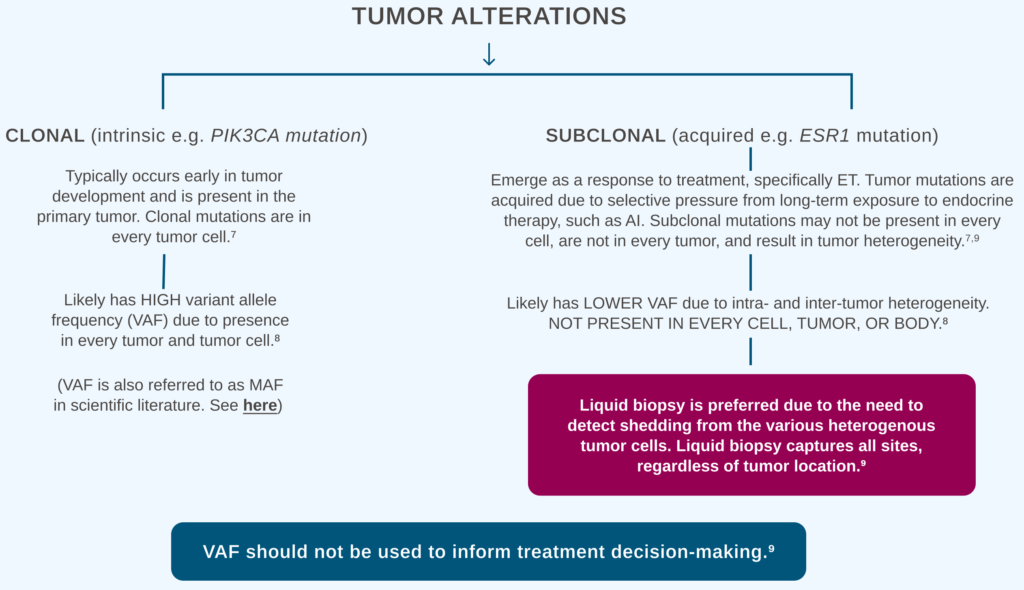
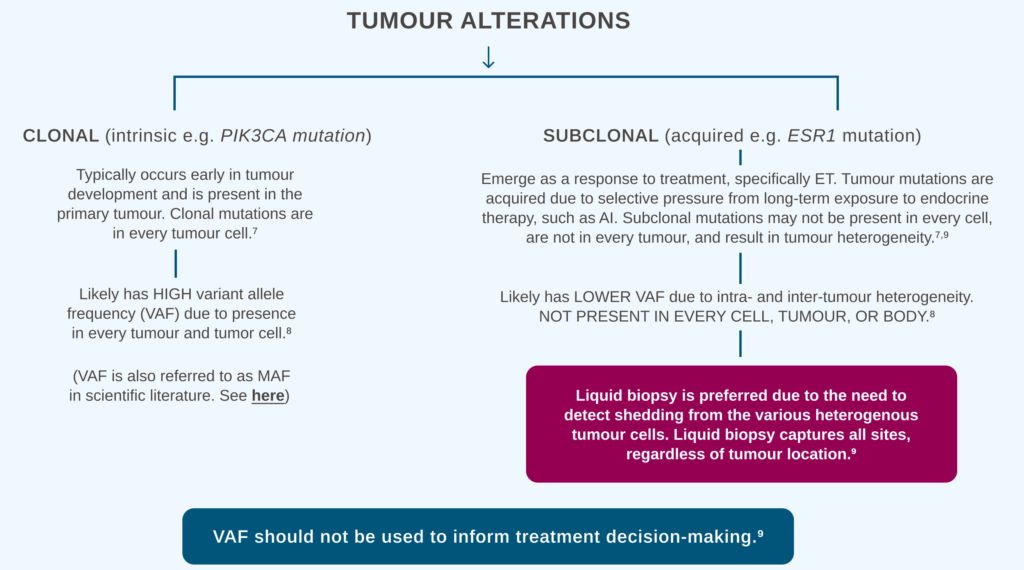
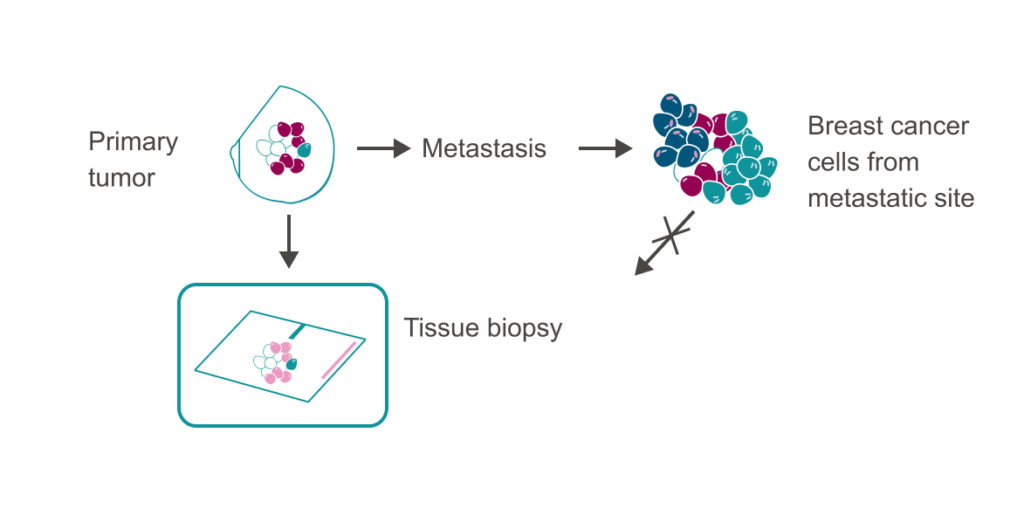
ESR1 mutations are subclonal (present in a subset of cells) and heterogenous within the tumour; therefore, it is possible that ESR1 mutations may not be detected in a tissue biopsy.*,3,4
ESR1 mutation testing can be performed either via liquid biopsy or fresh tissue biopsy.*,1,5,6
Liquid biopsy is recommended as the preferred method to detect ESR1 mutations due to a better ability to detect subclonal mutations.


UtilizeUtilise liquid biopsies for the detection of actionable mutations
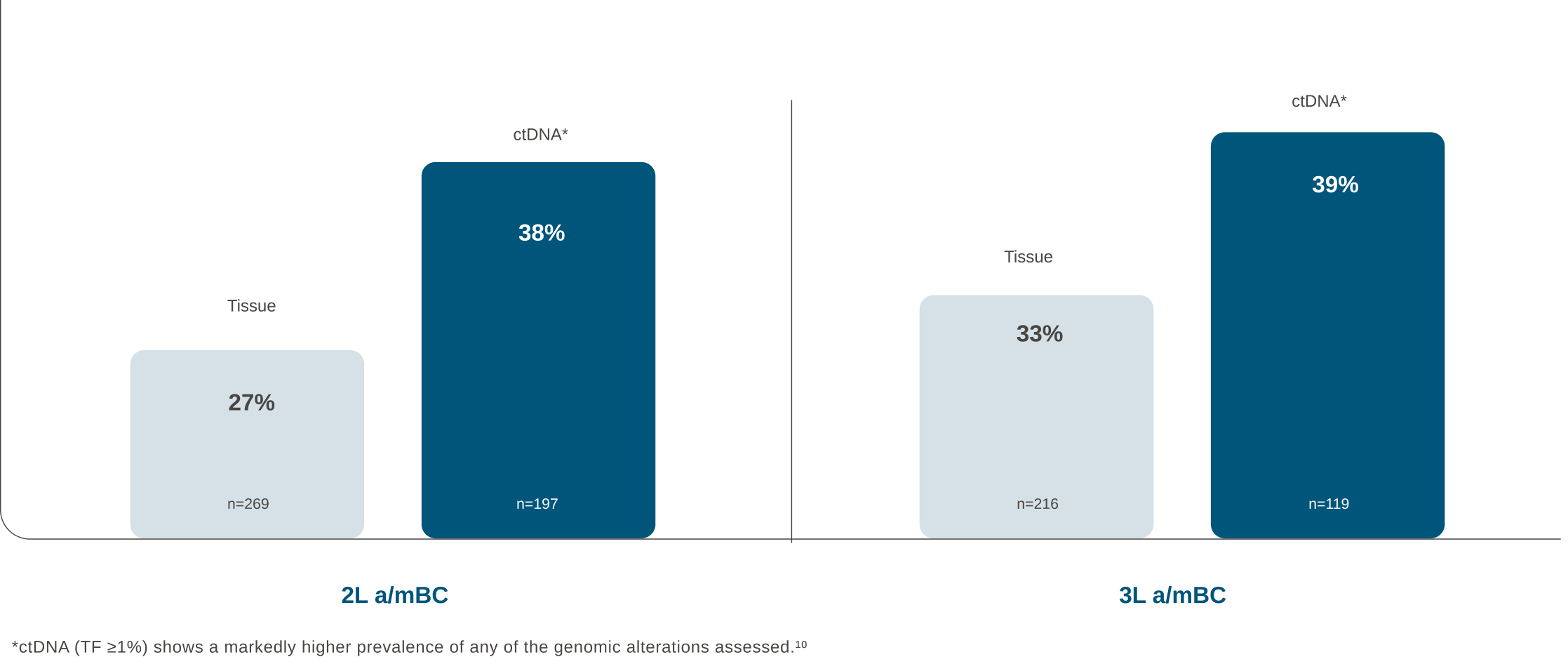
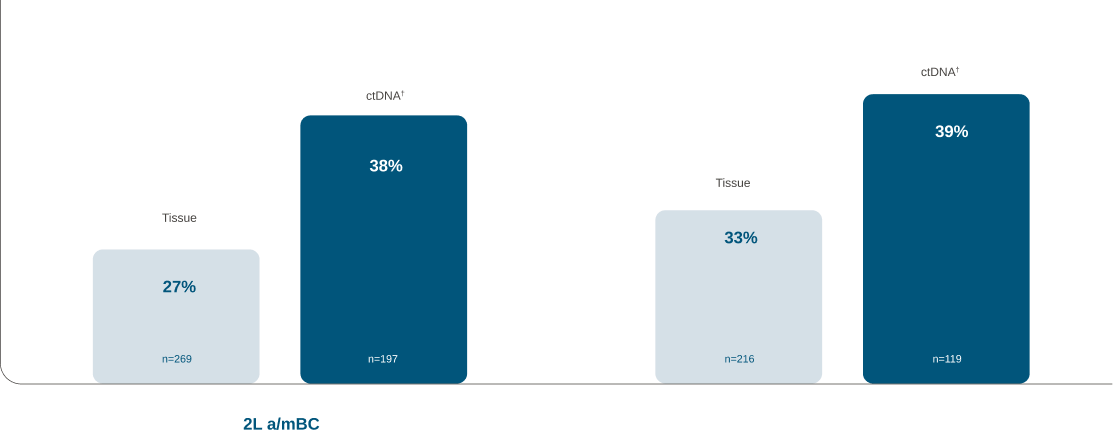
Prevalence of ESR1 mutations detected using ctDNA versus tissue biopsy* in 2L and 3L a/mBC10
*Fresh tissue biopsy testing is not reimbursed in the UK.
†ctDNA (TF ≥1%) shows a markedly higher prevalence of any of the genomic alterations assessed.10
Archived primary tumour tissue should not be used given the acquired nature of ESR1 mutations2
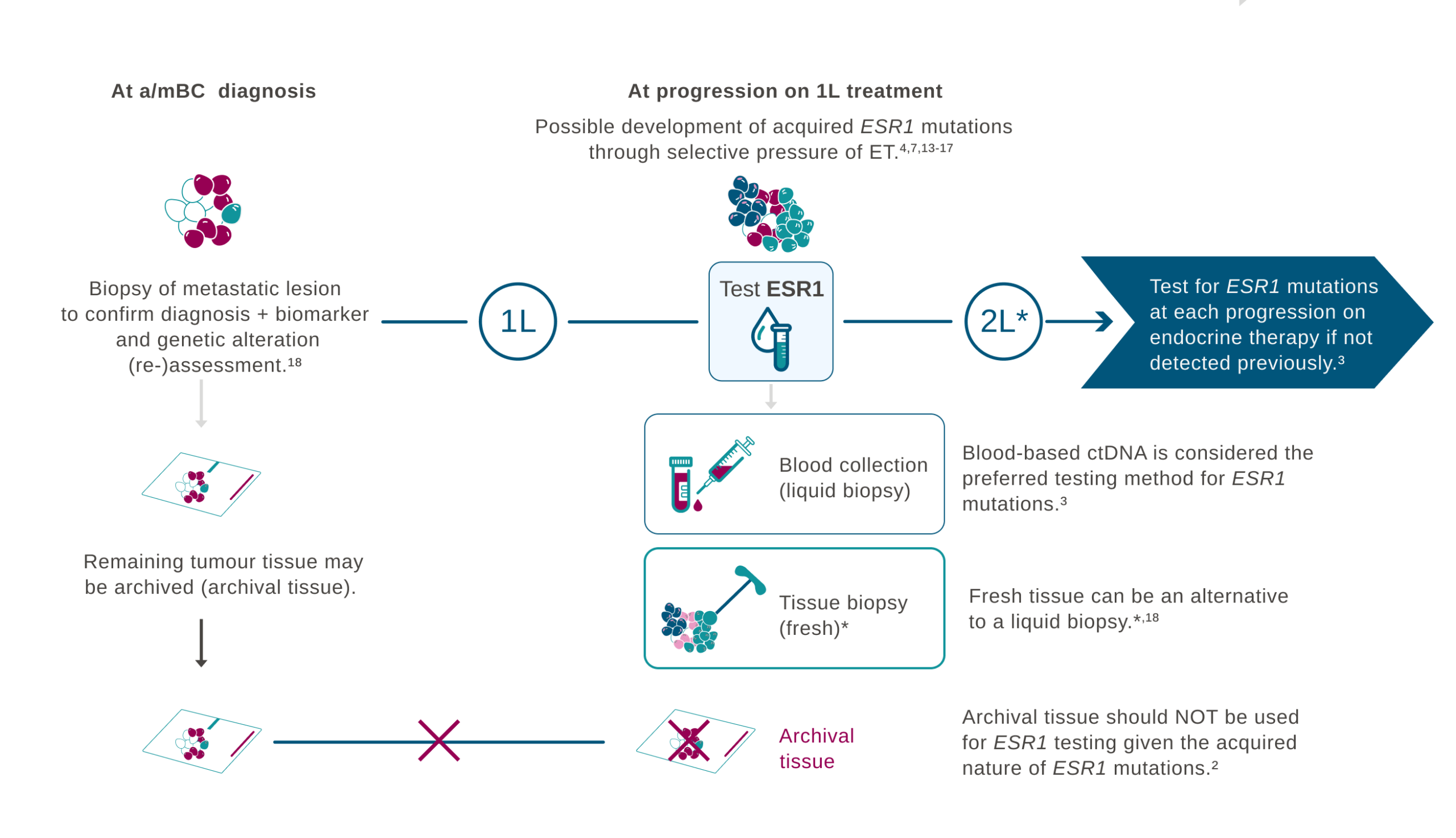
*Fresh tissue biopsy testing is not reimbursed in the UK.
Primary vs metastatic tumour biomarker testing
Biomarker testing in a/mBC may uncover mutational differences between the primary tumour and metastatic sites.19
Using only a tissue sample of the primary tumour for ESR1 testing may not capture mutations across all tumours, therefore missing the detection of an acquired ESR1 mutation at metastatic sites.2-4

Liquid biopsy <i>ESR1</i> quick testing guide
Preanalytics
Sample collection

Use specific ctDNA
collection tubes19-21

Use needles with
a large gauge diameter (≤21G)22

Fill up completely
to 10 ml21,23

Invert the tube 8-10x.
Do not shake24
Sample storage

Store at room
temperature until further processing20,22
Sample storage
Sample transportation

Best shipped within 3 days20
Best shipped within 1 day for arrival within 3 days20
Plasma preparation and ctDNA extraction
Best initiated within 3 day
after blood collection21
Preanalytical variables significantly impact the quality and quantity of isolated DNA, thereby affecting the performance of molecular tests. Therefore, the adherence to standardizedstandardised procedures is essential to ensure the validity of test results.21
Analytics

Use a validated dPCR
or NGS assay with
a limit of detection
(LOD) <1% VAF
sensitivity24-27
Reporting

Aim to report results
within 14 days of
sample receipt28
Please remember, in order to optimizeoptimise ESR1 testing in your ER+/HER2- a/mBC patients:

Test at EACH PROGRESSION on ET (if not detected previously)*,1,3,5,19

DO NOT USE primary archived breast cancer tissue2

USE LIQUID BIOPSY for high sensitivity3,4
*Repeat ctDNA testing may be approriate following a further line of endocrine therapy and subsequent disease progression as long as the previous test was negative and the patient remains eligible as per NICE recommendation (TA1036).
1L: first-line; 2L: second-line; 3L: third-line; AI: aromatase inhibitor; a/mBC: advanced/metastatic breast cancer; ctDNA: circulating tumour DNA; DNA: deoxyribonucleic acid; dPCR: digital polymerase chain reaction; ER+/HER2-: oestrogen receptor-positive, human epidermal growth factor receptor 2-negative; ESR1: oestrogen receptor 1; ET: endocrine therapy; LOD: limit of detection; mBC: metastatic breast cancer; NGS: next generation sequencing; PIK3CA: phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; VAF: variant allele frequency.
- Burstein HJ, et al. J Clin Onc. 2023;41(18):3423–5.
- Gradishar WJ, et al. J Natl Compr Canc Netw. 2023;21(6):594–608.
- Russano M, et al. J Exp Clin Cancer Res. 2020;39(1):95.
- Dustin D, et al. Cancer. 2019;125(21):3714–28.
- ESMO Metastatic Breast Cancer Living Guideline, v1.2 April 2025. Accessed March 2026. Available at: https://www.esmo.org/guidelines/living-guidelines/esmo-living-guideline-metastatic-breast-cancer.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast Cancer Version 4.2026. ©National Comprehensive Cancer Network, Inc. 2026. All right reserved. Accessed May 2026. To view the most recent and complete version of the guideline, visit NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
- Tarabichi M, et al. Nat Methods. 2021;18(2):144–55.
- Shin HT, et al. Nat Commun. 2017;8(1):1377.
- Bielo LB, et al. Trends Cancer. 2023;9(12):1058–68
- Bhave MA, et al. Breast Cancer Res Treat. 2024;207(3):599–609.
- Lone SN, et al. Mol Cancer. 2022;21(1):79.
- Pascual J, et al. Ann Oncol. 2022;33(8):750–68.
- Clatot F, et al. Breast Cancer Res. 2020;22(1):56.
- Chandarlapaty S, et al. JAMA Oncol. 2016;2(10):1310–15.
- Turner NC, et al. Clin Cancer Res. 2020;26(19):5172–7.
- Zundelevich A, et al. Breast Cancer Res. 2020;22(1):16.
- Schiavon G, et al. Sci Transl Med. 2015;7(313):313ra182.
- Gennari A, et al. Ann Oncol. 2021;32(12):1475–95.
- Lee N, et al. Int J Mol Sci. 2020;21(22):8807.
- Ignatiadis M, et al. Nat Rev Clin Oncol. 2021;18(5):297–312.
- Danesi R, et al. Clin Chim Acta. 2021:520:168–71.
- Meddeb R, et al. Clin Chem. 2019;65(5):623–33.
- Nikolaev S, et al. Anal Biochem. 2018;542:34–9.
- Lee JS, et al. Ann Lab Med. 2024;44(3):195–209.
- Najim O, et al. Front Oncol. 2023;13:1221773.
- Garcia J, et al. Oncotarget. 2018;9(30):21122–31.
- Mattox AK, et al. Oral Oncol. 2022;128:105805.
- Lee Y, et al. JCO Precis Oncol. 2020:4:PO.20.00121.